Research and technology
Histological studies have enabled us to verify the new functions of the Timed TD50 micropulse.
-
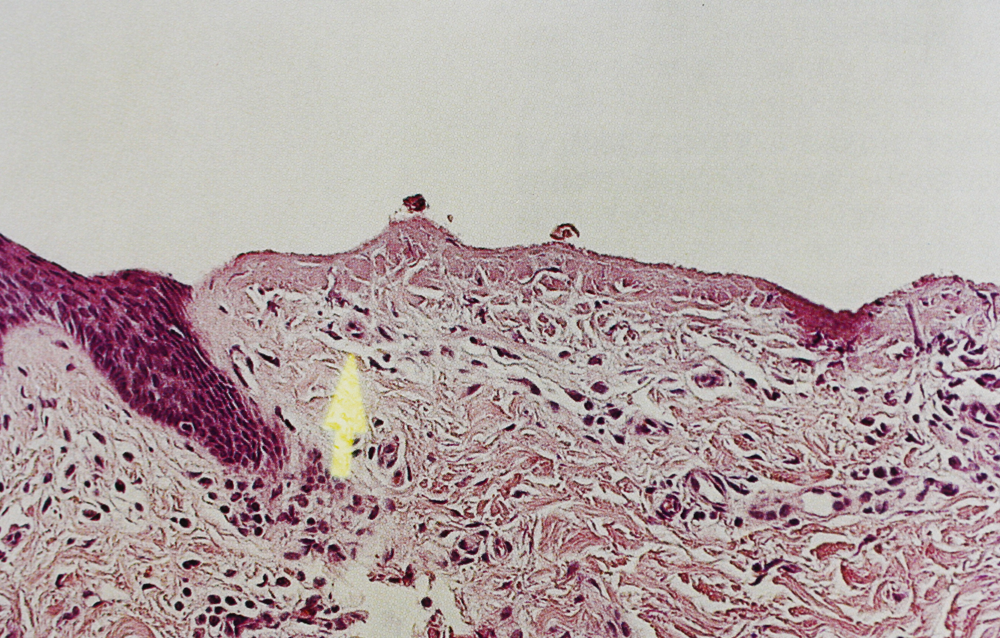
- Skin de-epithelialised by means of the specific Timed function. The arrow indicates the integrity of the capillary-papillary complex.

-
- Pulsed Timedsurgical cutting. Absence of burning at the edges. A hairbulb cut in half can be seen.

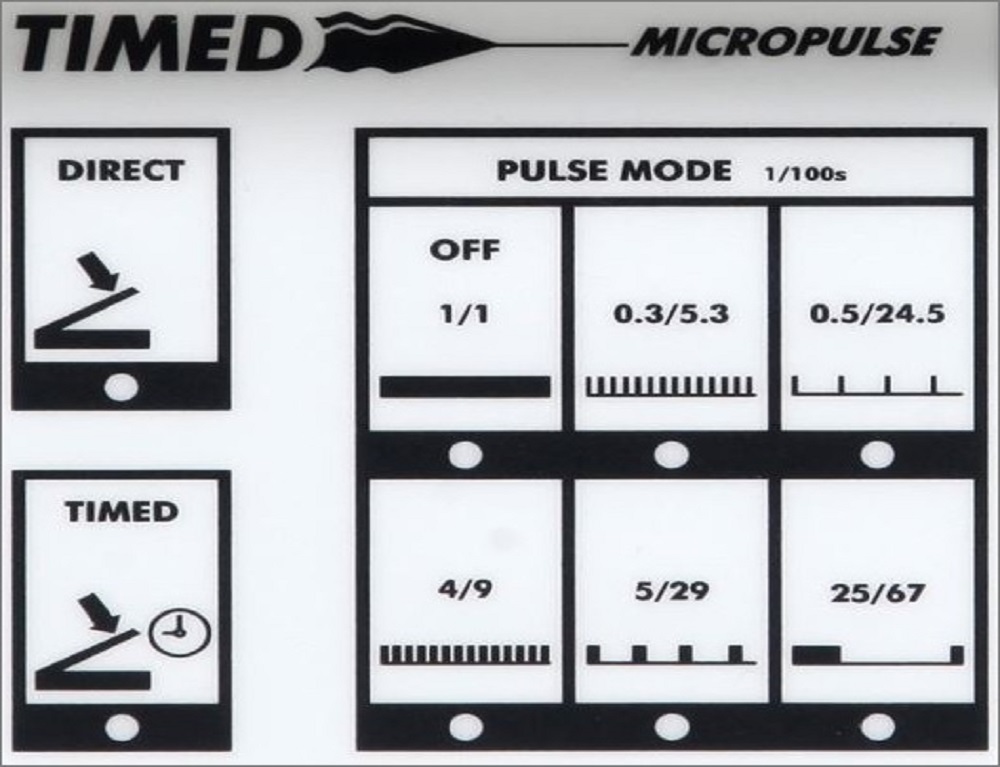
| 25/67 | Rapid definitive depilation |
| 5/29 | Teleangiectasias and Microteleangiectasias |
| 4/9 | Pulsed timedsurgical de-epithelialisation |
| 0,5/24,5 | Slow pulsed cutting – Fractional mixed peeling |
| 0,3/5,3 | Rapid pulsed cutting – Resurfacing (Coag) |
The Timed TD50 micropulse provides precise control over the parameters that condition the effect of a high-frequency current in the tissues. The Timed TD50 micropulse is endowed with a power system designed to be programmable, stable power indicated in Watts, and emission duration control. The various types of procedure are performed by means of specially programmed currents.
Each procedure utilises specific standardised programme data and a specific electromaniple. The perfectly reproducible settings of the Timed, together with selection of the appropriate function, enable the effects of a diathermal emission to be predicted. This means that the programme data from a set of case-records can be retrieved and made available to other operators working on similar cases.
The programme data and the operating techniques of each specific procedure make it easy to perform procedures that could formerly be carried out only by expert operators, if at all.
Programmed diathermosurgery has been made possible by the Timed apparatus, its electrodes, its power system that is proof against electromagnetic interference, its discretized power scale control, and the controls needed by a programmable apparatus.
The research conducted by Korpo has led to the creation of special electromaniples and electrodes with flexible conical and triangular tips. These electromaniples, together with the specific currents, have made it possible to carry out slow and rapid pulsed timed cutting. This cutting technique does not burn the edges of the cut and is perfectly controllable. As the pressure exerted on the tissues is negligible (less than 5 g), precise micro-excisions can be performed; for instance, a skin flap can be cut out between two 1 mm lines. Full-thickness skin and mucosal excisions performed by means of timed or slow or rapid pulsed cutting are practically bloodless, can be sutured and heal rapidly. In upper blepharoplasty, for example, the stitches are removed after only three days. If a scalpel is used to perform the same operation, the stitches cannot be removed in less than a week.
-
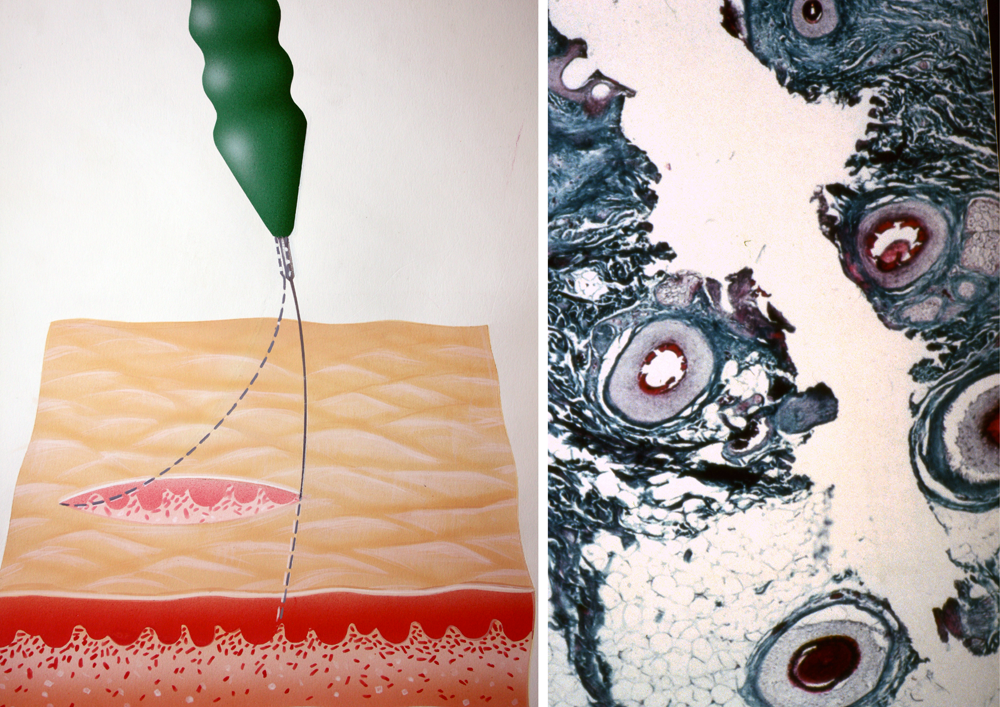
- When incisions are made by means of pulsed timedsurgical cutting, the pressure exerted on the tissues is less than 5 g.

-

- A colour code indicates the diameter of the electromaniples

-
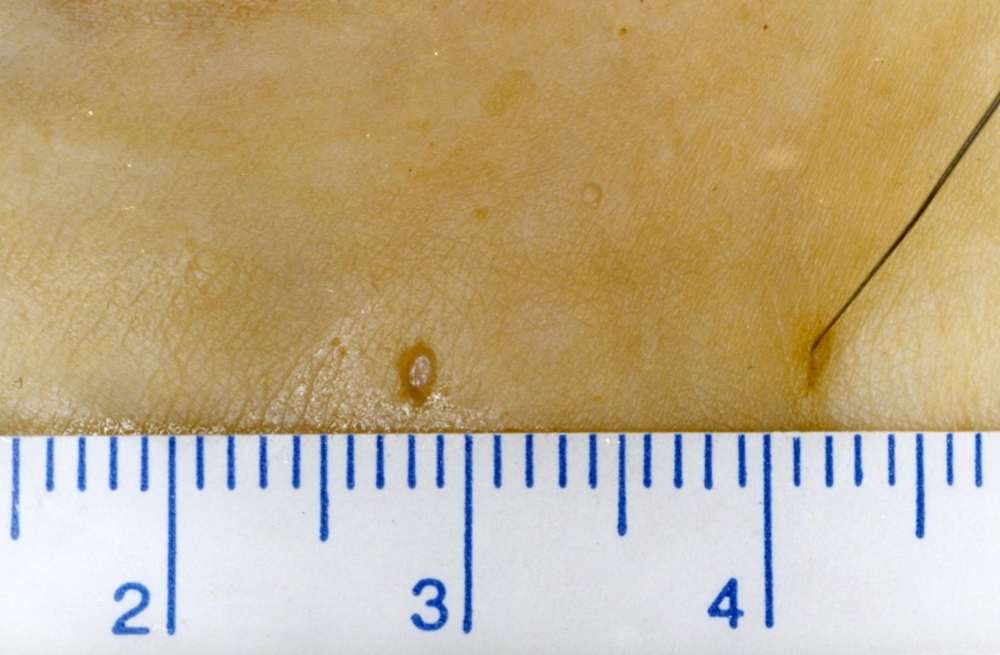
- Timedsurgical cutting enables a skin flap to be cut out between two 1 mm lines.

Two EM 10 electromaniples with a partially isolated electrode enable the ascending artery of a stellate angioma to be coagulated underneath the skin where it originates. This bipolar technique does not leave any scars on the skin.
The electromaniples are colour-coded according to the diameter of their electrodes. Tiny differences in diameter, even of just one-hundredth of a millimetre, which are indistinguishable to the naked eye, produced different clinical effects.
| Electromaniples | Diameter | Applications |
|---|---|---|
| EM 10 White | 0,08 mm | Rapid pulsed and slow pulsed cutting of skin and mucosa, fine micro-telangiectasias, depilation of fine hair on the upper lip |
| EM 10 Green | 0,10 mm | Electroshaving, rosacea (micro-telangectasias), definitive depilation, subcutaneous cutting |
| EM 10 Grey | 0,15 mm | Telangiectasias of the face and body, Electroshaving, definitive depilation of the body, excision of pedunculated fibromas, subcutaneous cutting |
| EM10 Yellow | 0,20 mm | De-epithelialisation (edge of angle), excision of pedunculated fibromas |
| EM 10 Black | 0,30 mm | Surgery |
| EM 15 | 1,5 mm | Resurfacing, micro-vaporisation, vaporisation of benign neoformations, coagulation of viral warts, coagulation of blood vessels, cleansing and “sterilisation” of ulcers |
| Insulated electromaniples | Diameter | Applications |
|---|---|---|
| EM 10 Green Insulated | 0,10 mm | Bipolar coagulation of the ascending artery of stellate angiomas. Elimination of malar bursae, small subcutaneous excesses correction |
| EM10 Grey Insulated | 0,15 mm | Bipolar coagulation of the ascending artery of stellate angiomas. Elimination of malar bursae, small subcutaneous excesses correction |
History
In 1900, Rivière demonstrated that, at equal power, the lesional effect is greater if a smaller electrode is used, since the current density is greater.
In 1907, Keating-Hart and Pozzi coined the term “fulguration” (from the Latin fulgor) to indicate the superficial charring that is produced when a modest mono-terminal high-frequency current at high tension creates sparks in the air between the electrode and the tissue.
In 1907, Forest patented the triode, and in 1908 became the first to achieve a cutting effect with a current generated by a cathode tube.
In 1909, using a bi-terminal apparatus with low tension and high current Doyen produced a much higher temperature than had previously been reached (500 C¡). In 1911, Clark distinguished electro-coagulation from fulguration.
In 1924, Wyeth and Clark demonstrated the characteristics of a modulated high-frequency current, in comparison with an unmodulated current, and the different effects of each on the tissues.
In 1926, Wyeth designed the first electro-scalpel able to develop a cutting current; he called this instrument an endothermal knife.
In 1928, Bovie described an apparatus that combined cutting and coagulation, and which could control bleeding more effectively.
In 1940, Grenwood invented an important accessory: bipolar pincers, i.e. connected to both outputs of the diathermal generator. This was the beginning of bipolar coagulation, which is used in microsurgery and is indispensable in neurosurgery.
In 1958, Malis developed a bipolar diathermocautery with a floating patient circuit, i.e. completely insulated from the electrical source feeding the apparatus; this development greatly increased safety.
In the 1970s, apparatuses with spark gaps and valves began to be replaced by those with transistors, which were more accurate and reliable.
At the end of the 1970s, programmed diathermosurgery was invented and the first programmable diathermocautery was made (Capurro 1979, USA patent).
In the middle of the 1990s, after having enabled numerous techniques to be carried out, programmed diathermosurgery acquired the medical-scientific support needed in order to communicate this knowledge in an organic manner, thereby giving rise to Timedsurgery. In 2010, the scientific department of Korpo patented the rotating electrodes used in Electroporo-Cosmesis.
Visit the Timedsurgery section of the Medical Video Journal www.crpub.org ISSN 1971-8152